
Your Daily Meds - 28 November, 2022
Your Daily Meds - 28 November, 2022

Good morning and welcome to your Monday dose of Your Daily Meds.
Case:
A middle-aged male with a known history of peptic ulcer disease presents to the Emergency Department complaining of severe, sudden onset epigastric pain. On examination, there are signs of peritonism and he is haemodynamically unstable. His erect chest/abdominal x-ray is shown below:
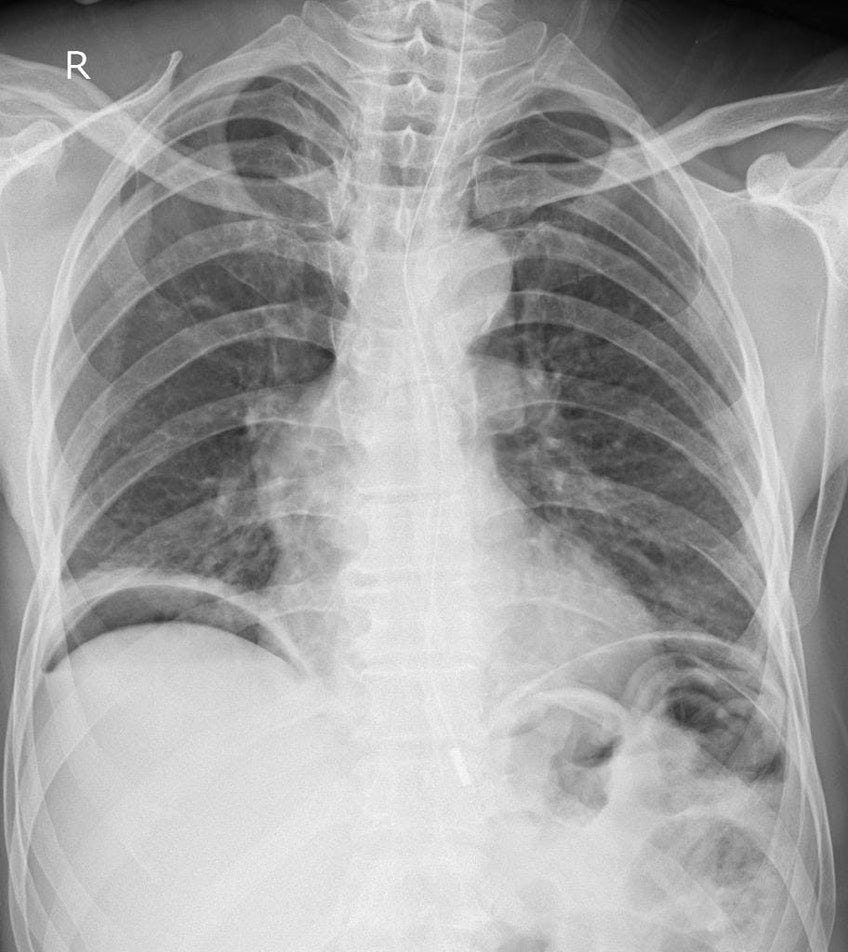
Given this man’s history, examination and imaging findings, where is the likely causative lesion?
Gastro-oesophageal junction
Cardia
Fundus
Body of stomach
Pylorus
Have a think.
Scroll for the chat.
Case:
A 12-year-old female presents to the Emergency Department complaining of severe wrist pain. She reports falling onto an outstretched hand while playing netball. On examination, there is reduced range of movement in all directions due to pain and exquisite tenderness in the anatomical snuffbox. Her x-ray is shown below:

Which of the following conditions is this girl at most risk of given this pathology?
Osteoporosis
Avascular necrosis
Osteomyelitis
Ligamentous instability
Osteoarthritis
Have a think.
Scroll for the chat.
Perf-ed:
The x-ray shows free gas under both domes of the diaphragm.
Given that this man has a history of peptic ulcer disease and signs of peritonitis, the main concern would be an acutely perforated ulcer.
This would allow a communication between the stomach or duodenum with the peritoneal space, irritating the peritoneum and causing peritonitis.
Approximately 80% of perforations due to peptic ulcer disease occur in the region of the pylorus and first part of the duodenum. Thus, given the options, the pylorus is the most likely location for the lesion.
Head to Radiopaedia for good images and cases like this.
Cracked:
Key to answering this question is recognising the likelihood diagnosis of scaphoid fracture based on the history, examination and radiological findings. Avascular necrosis of the scaphoid occurs in approximately 30% of cases and is more likely in cases of displaced fracture. Avascular necrosis is relatively common as the scaphoid has a retrograde blood supply that enters the bone distally.
Less severe complications of scaphoid fracture include non-union or malunion of the fracture causing instability and secondary arthritic change.
Ligamentous instability can occur, especially in response to displaced and angulated fractures, however osteoporosis is less likely as a complication.
Osteomyelitis is an unlikely complication of a simple undisplaced scaphoid fracture.
Bonus: What fluid loss can occur via sweating?
Answer in tomorrow’s dose.
News: I made a little Ward Call Course for you all. It maps out an Evening Ward Call shift and covers a bunch of common tasks that you may need to do, like:
Deteriorating Patients
Heparin Infusions
Fluid Orders
Electrolyte Replacement
Difficult patients - Discharge Against Medical Advice, Ryan’s Rule
End of Life etc
You can find the course page here:
It’s free and always will be. Let me know what you think.
Remember, you are free to rip these questions and answers and use them for your own flashcards, study and question banks.
As always, please contact me with any questions, concerns, tips or suggestions. Have a great day!
Luke.